An Unexpected Finding: Interpreting Markedly Low LDL Cholesterol
Dr Faiza Jamal, Resident III
Dr Aysha Habib Khan, Professor
Section of Chemical Pathology
It began as a routine laboratory evaluation for a 52-year-old male patient who had no specific complaints and no significant past or family history. His biochemical profile was largely unremarkable except his LDL cholesterol was reported as 7 mg/dL, an unusually low value prompted the referring physician to seek further clarification from the laboratory regarding the clinical significance and possible causes of such markedly low LDL levels.
Given the unexpected nature of the result, the sample was rechecked, and a repeat analysis was sent to another laboratory for confirmation. The findings returned unchanged: persistently very low LDL levels. To better understand this, lipoprotein electrophoresis was performed. The pattern was peculiar but consistent there was a markedly reduced β-band, corresponding to LDL, while the pre-β band, representing VLDL, remained preserved.
This distinction proved crucial. In disorders where both VLDL and LDL are reduced, the underlying issue often lies in impaired hepatic production of lipoproteins. However, in this patient, the preservation of the pre-β band suggested that the liver was producing VLDL adequately. The abnormality, therefore, appeared to lie either in the conversion of VLDL to LDL or in an increased clearance of LDL from circulation as shown in the figure.
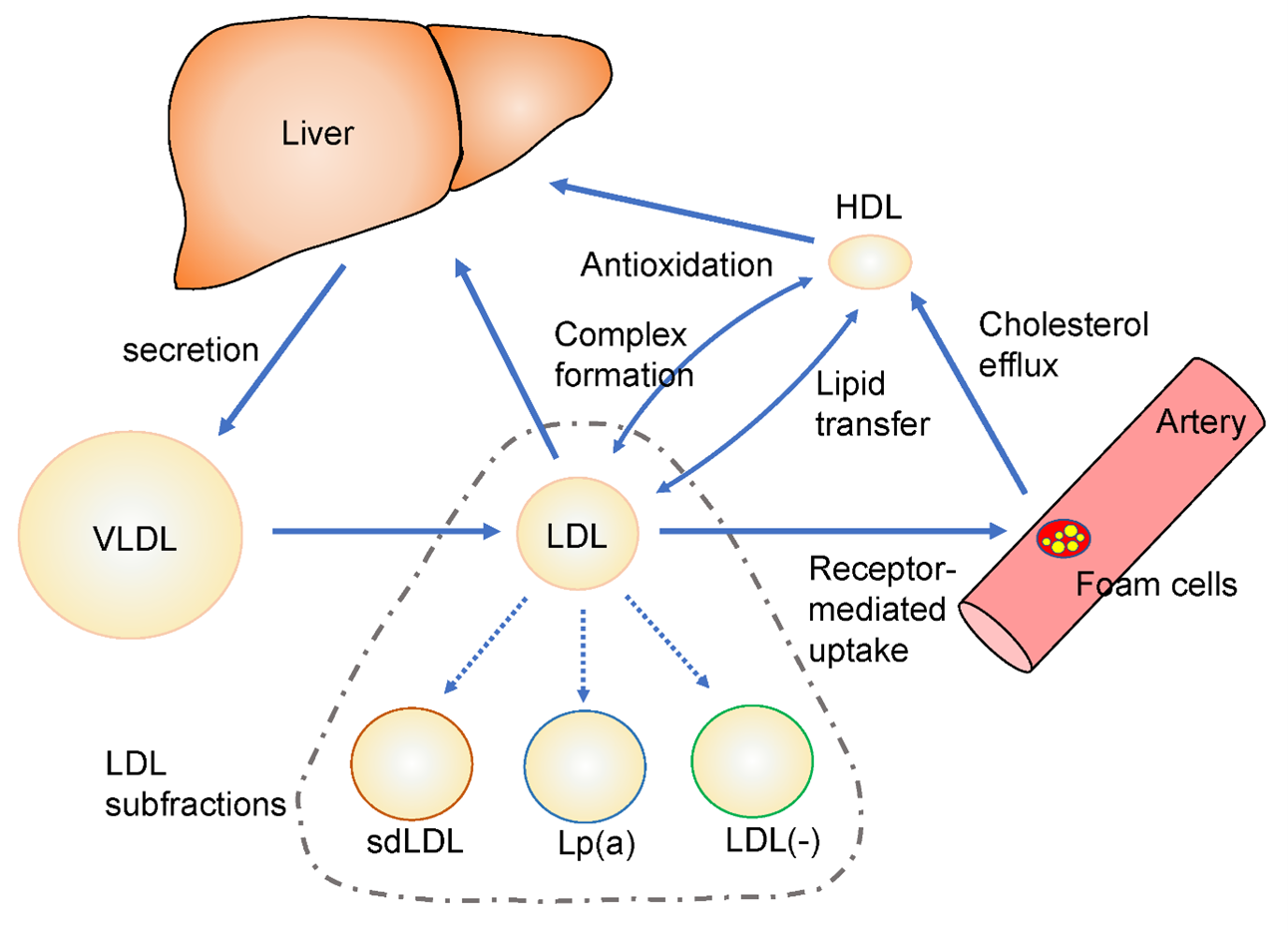
Figure 1: Metabolic Pathways of VLDL, LDL, and HDL Lipoproteins
With no symptoms to guide the diagnosis, attention turned to possible underlying causes. Secondary conditions such as hyperthyroidism, chronic illness, liver disease, or malnutrition were considered, but there was no clinical or laboratory evidence to support them. The absence of drug history further narrowed the possibilities. What remained most likely was a primary, genetically determined state either a mild form of familial hypobetalipoproteinemia or a variant involving enhanced LDL receptor activity, such as PCSK9 loss-of-function. Both conditions are known to produce very low LDL levels while leaving patients otherwise healthy. Table 1 outlines the category of conditions associated with low LDL levels along with their cause, mechanism and key clinical clues.
Table 1: Categorization of Different Causes of Low LDL
| Category | Cause | Mechanism | Key Clinical Clues |
| Physiological / Benign | Genetically low LDL (e.g., Familial Hypobetalipoproteinemia) | Reduced ApoB production → decreased LDL formation | Asymptomatic, family history, persistently low LDL |
| | PCSK9 loss-of-function variants | Increased LDL receptor activity → enhanced LDL clearance | Very low LDL, cardioprotective, no symptoms |
| Endocrine | Hyperthyroidism | Increased LDL receptor expression and cholesterol metabolism | Weight loss, tachycardia, low TSH |
| Hepatic | Chronic Liver Disease | Impaired lipoprotein synthesis | Abnormal LFTs, jaundice, coagulopathy |
| Nutritional | Malnutrition / starvation | Reduced substrate for lipoprotein synthesis | Low BMI, poor intake |
| | Malabsorption syndromes | Impaired fat absorption | Diarrhea, steatorrhea, vitamin deficiencies |
| Chronic Illness | Chronic infections (e.g., tuberculosis) | Increased catabolism, cytokine effects | Fever, weight loss |
| | Malignancy | Increased metabolic demand and cytokine-mediated effects | Cachexia, systemic symptoms |
| Genetic (Severe) | Abetalipoproteinemia | Absence of ApoB → no chylomicrons, VLDL, LDL | Fat malabsorption, neurological signs, vitamin deficiencies |
| Medications | Statins | Inhibit cholesterol synthesis → upregulate LDL receptors | Drug history present |
| | PCSK9 inhibitors | Markedly increase LDL clearance | Very low LDL, therapeutic context |
| | Other lipid-lowering drugs (e.g., ezetimibe) | Reduced cholesterol absorption | Medication history |
| Acute/Other | Acute illness / inflammation | Transient reduction in lipid levels | Recent illness, hospitalization
|
Interestingly, such lipid profiles are often associated with a reduced risk of atherosclerotic cardiovascular disease, making them, in many ways, biologically advantageous. Unlike more severe disorders of lipoprotein metabolism, this pattern does not typically interfere with triglyceride transport or energy balance. The feared complications of fat-soluble vitamin deficiency or neurological involvement are generally absent in these milder forms.
For this patient, the finding ultimately shifted from being a cause for concern to a point of clinical curiosity. No active intervention was required. Instead, a strategy of periodic monitoring was adopted, with attention to maintaining a balanced diet and general health. The case served as a reminder that not all abnormal laboratory values signify disease some reflect the wide and fascinating spectrum of human metabolic variation. Table 2 highlights the approach to patients identified with low LDL along with key clinical clues for a practitioner to help in managing these cases.
Table 2: Approach to Very Low LDL Cholesterol (<40 mg/dL)
| Section | Key Points for GPs |
| Definition | LDL cholesterol <40 mg/dL (very low);
<20 mg/dL is rare and warrants evaluation |
| Initial Step | Always confirm the result (repeat test ± alternate lab) to exclude analytical error |
| Clinical Context | Assess if patient is symptomatic or asymptomatic; review history and medications |
| Common Secondary Causes | • Hyperthyroidism • Chronic illness/infection • Liver disease • Malnutrition/malabsorption • Malignancy • Lipid-lowering therapy (e.g., statins, PCSK9 inhibitors) |
| Primary (Genetic) Causes | • Familial hypobetalipoproteinemia (FHBL) • PCSK9 loss-of-function variants • Abetalipoproteinemia (rare, usually symptomatic) |
| Clues from Lipid Profile | • Low LDL + normal VLDL/TG → increased LDL clearance or conversion issue • Low LDL + low TG → impaired lipoprotein production |
| When to Investigate Further | • LDL <20 mg/dL • Presence of symptoms (neurological, steatorrhea) • Family history of lipid disorders • Suspicion of systemic disease |
| Useful Tests | • Full lipid profile (including triglycerides) • Liver function tests • Thyroid function tests • Consider lipoprotein electrophoresis • Genetic testing (if indicated) |
| Clinical Significance | • Often benign or protective (reduced cardiovascular risk) • Severe genetic forms may be associated with fat-soluble vitamin deficiency (rare in mild cases) |
| Management | • If asymptomatic and secondary causes excluded → no treatment required • Monitor periodically • Ensure balanced nutrition |
| When to Refer | • Unexplained very low LDL (<20 mg/dL) • Suspected genetic lipid disorder • Presence of systemic or neurological symptoms
|
In an era where elevated cholesterol dominates clinical concern, low cholesterol levels require equally careful interpretation. Rather than being inherently beneficial, hypocholesterolemia may reflect physiological variation, genetic factors, or efficient lipid metabolism, sometimes indicating a potentially protective state.
However, it can also arise secondary to underlying conditions such as malabsorption, hyperthyroidism, liver disease, or systemic illness. Given cholesterol's essential biological roles, values at either extreme should always be interpreted within the broader clinical context.