Grand Round: The direct and indirect effect of pneumococcal vaccines in decreasing invasive disease and carriage in the paediatric population of Pakistan
Epidemiologist Dr Imran Nisar was one of the researchers who have been instrumental in studying the pneumococcal vaccine in Pakistan. This talk was recorded from his Grand Round delivered on February 14, 2024 at the Department of Paediatrics & Child Health at AKU, Karachi.
.png)
Pneumococcal can cause both invasive and non-invasive disease. It is covered by different vaccine formulations across the globe and there can be remarkable geographic variation in coverage.
PCV 10 covers more than 70% of the invasive pneumococcal disease globally. Some countries have PCV 10 and others PCV 13.
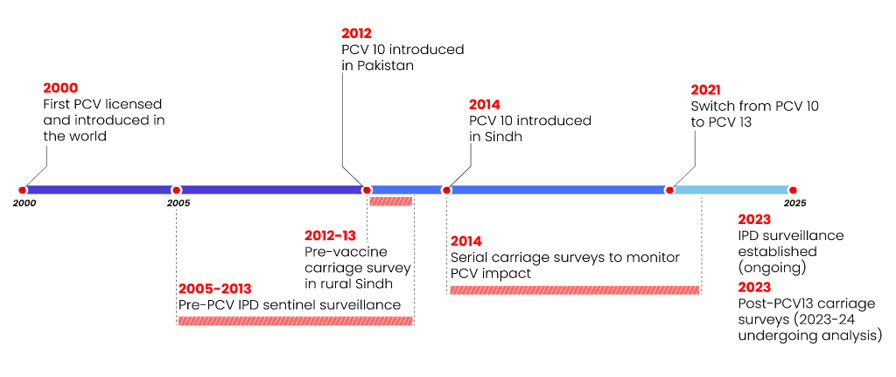
Timeline of select published work by AKU faculty
2009: Surveillance of Pneumococcal Meningitis among Children in Sindh, Southern Pakistan
2014: Pneumococcal Serotypes and Serogroups Causing Invasive Disease in Pakistan, 2005–2013
2018: Nasopharyngeal carriage of Streptococcus pneumoniae in children under 5 years of age before introduction of pneumococcal vaccine (PCV10) in urban and rural districts in Pakistan
2019: Effectiveness of 10-valent pneumococcal conjugate vaccine against vaccine-type invasive pneumococcal disease in Pakistan
Introduction of a vaccine
Before you introduce a vaccine, you have to make sure that it works in your population. Trials are held with the assumption that the incidence of the disease will go down in vaccinated people. This helps evaluate a vaccine's impact.
You need to set up a surveillance system to see the number of cases go down.
We set up a surveillance system across 18 hospitals in Sindh, southern Pakistan (from 2007-08). There were 2,690 children with suspected meningitis who were enrolled.
We had out of close to 2,600 CSF samples, 412 were purulent. Majority of them, close to 60% were haemophilus influenzae Type B followed by streptococcus, and a small percentage of Neisseria.
Pakistan was the first country in South Asia to introduce the Hib vaccine in its EPI.
Some of the follow-up work was done to then serotype these pneumococcal isolates which were causing the invasive disease. These are pneumococcal serotyping which was done on 111 IPD isolates. Two-thirds of them, or 65%, are covered by the 10 valence vaccine and an additional 2% is covered by the PCV 13, which have three other serotypes 3, 6a and 19a. The remaining 33% are the non-vaccine zero types.
On top of that we did a carriage survey. The first big finding from that was that if you swab infants or children under the two years of age and test them for Pneumococcus, 80% of them are carrying Pneumococcus in their nasopharynx. In the general population it comes down to 40-50% in adults. But it's very, very high in our population as compared to a lot of western population. For example, in the paediatric population in US it's 4% to 5% of nasopharyngeal carriage.
We serotyped them to see that how much coverage is there of different vaccine formulations: 33% were covered by PCV10 and additional close to 20% were covered by PCV13 and the remaining almost 50% were non-vaccine serotypes.
Pakistan introduced the 10 valent pneumococcal vaccine in its EPI in 2012 and it's given 6, 10, 14 weeks. We switched in 2021 to PCV 13.
In the beginning of 2004, in the first year of the study vaccine coverage was 41%. By the time we finished the study, the vaccine coverage had risen up to, for the three doses of pneumococcal vaccines, to nearly 70%.
We compare with age appropriate vaccination versus unvaccinated. Again you see 6A, 19A are the highest number of isolates present. The remaining are the non-vaccine serotypes.
The PCV10 carriage declined from 19.9% in the beginning to 13.2% towards the end of the study.
We saw a 34% reduction in vaccine type carriage in the vaccinated group compared to the unvaccinated group in the post-introduction phase.
We saw a high overall pneumococcal carriage in the study population. Three doses were 40% effective. PCV13-specific serotypes and 60A and 19A contributed to significant burden of carriage and there was an increase in the prevalence of 19A in the post-introduction phase.
This transcript has been shortened and edited.